C-Section Shelf (C-Section Pouch): Why It Happens and How to Fix the Lower Belly Bulge
Why your stomach may still look pregnant after a C-section — and what can be done about it
Dr Varun Harish, FRACS Plastic Surgeon
First published:
Many women notice a persistent lower abdominal bulge, pouch, or “shelf” after a C-section that does not improve with time, exercise, or weight loss. A C-section shelf is a lower abdominal overhang that forms above a C-section scar, most commonly caused by scar tethering, excess skin, or abdominal muscle separation after pregnancy. This is also referred to as a C-section pouch or overhang above the scar, and may develop as a more general post-pregnancy abdominal prominence that often does not resolve with time, exercise, or weight loss.
Understanding why these changes occur is important, because different underlying causes require different treatments. This article outlines the most common anatomical reasons for post-pregnancy abdominal contour changes and explains how surgeons distinguish between problems related to the scar, skin, fat, and abdominal muscles. These distinctions are important, as treatment options such as scar revision, muscle repair, or abdominoplasty (tummy tuck) are tailored to the underlying anatomy.
Patients in Sydney and the North Shore frequently seek assessment for persistent abdominal contour changes after pregnancy.
Questions about cost and Medicare eligibility are also common.
This article’s content reflects common findings seen in post-pregnancy and post-caesarean patients assessed in clinical practice, where multiple anatomical factors often contribute to lower abdominal contour changes.
What is a C-section pouch or overhang?
A C-section pouch (also called a C-section shelf or overhang) is a lower abdominal bulge that forms above a Caesarean section scar. It most commonly occurs due to scar tethering, excess skin, or abdominal muscle separation after pregnancy.
 At a glance: what may be causing your abdominal bulge after pregnancy?
At a glance: what may be causing your abdominal bulge after pregnancy?
| Cause | Typical feature |
|---|---|
| Scar tethering | Bulge is localised directly above the C-section scar and the scar feels fixed |
| Diastasis recti | Bulge runs along the middle of the abdomen and worsens with straining or sit-ups |
| Loose skin | Skin folds or hangs when bending forward |
| Hernia | Bulge increases with cough/strain, or is painful |
Why does a C-section shelf or C-section pouch occur after pregnancy?
A post-pregnancy abdominal bulge is rarely due to a single factor. Patients sometimes describe this appearance as a C-section overhang, referring to the fold of tissue that develops above the scar. In most cases, it reflects a combination of scar behaviour, skin changes, muscle separation, and residual fat. Understanding these contributors is essential before considering treatment.
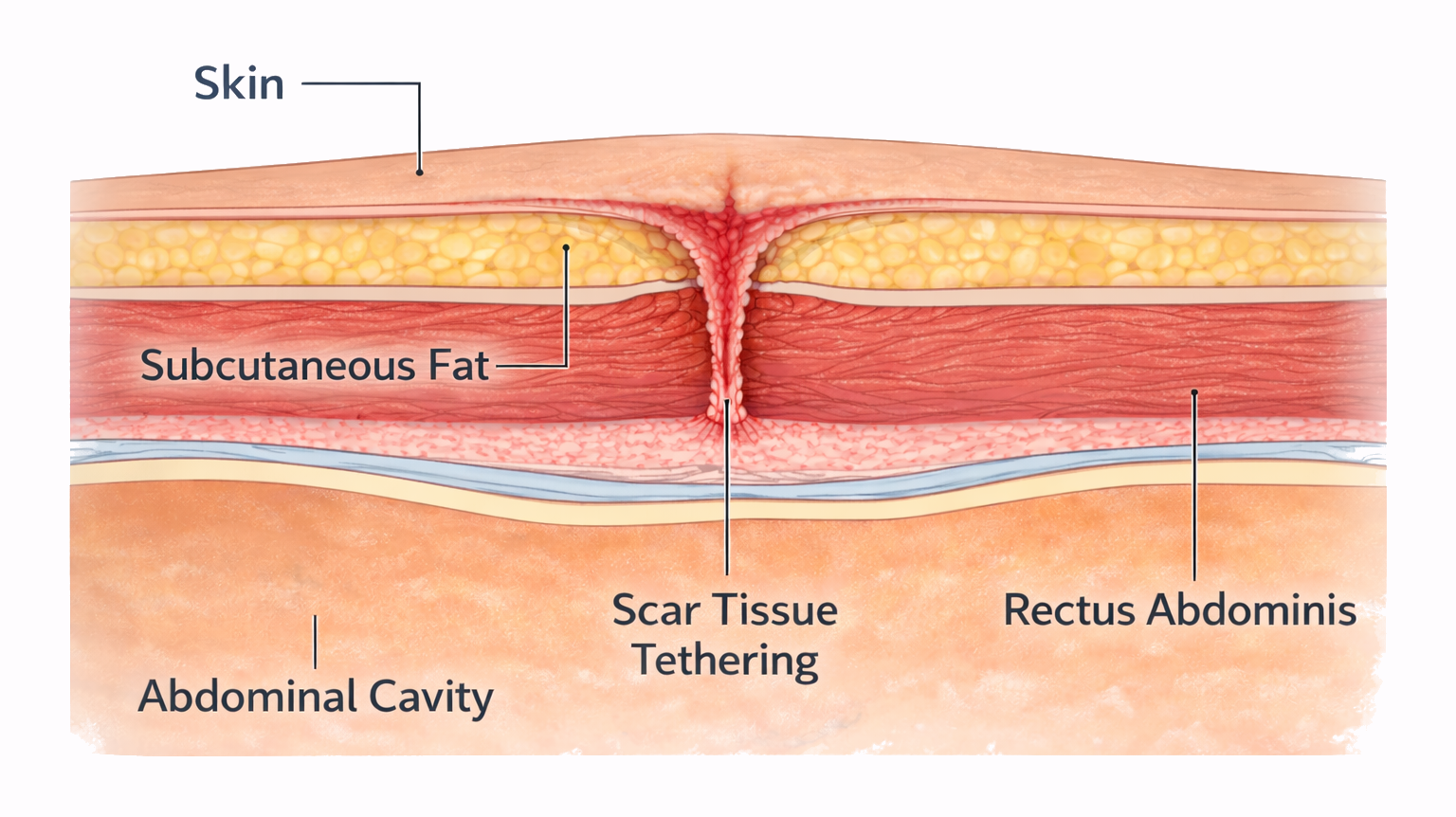
How a C-section shelf forms
Scar tissue forms along the lower abdomen.
Healing tissue may tether the skin to the abdominal wall beneath it.
While surrounding tissue moves normally, the scar remains anchored.
When sitting or bending, the tissue above this fixed point can fold forward, producing the visible shelf.
C-section scar tethering (C-section ‘shelf’ or ‘pouch’)
After a C-section, the skin incision heals by forming scar tissue. In some patients, this scar becomes tethered or stuck to deeper layers of the abdominal wall, anchoring the skin at the scar line. The skin and soft tissue above the scar may then protrude slightly, creating a visible ledge or “shelf”.
The important features of a C-section shelf or pouch include:
- The bulge is localised directly above the scar
- The upper abdomen may otherwise feel relatively flat
- Weight loss or exercise has little effect on the shelf
- A scar that may appear indented, tight, or adherent
In these cases, the bulge often looks more prominent when sitting or bending because the scar stays fixed while the tissue above it folds forward. Importantly, bulges caused by scar tethering are different from abdominal muscle separation, and require a different surgical approach.

A C-section shelf is most often caused by scar tethering at the incision site, sometimes combined with skin laxity or muscle separation, rather than by fat alone.
For more information about scarring and treatments available, see our Scar Revision page.
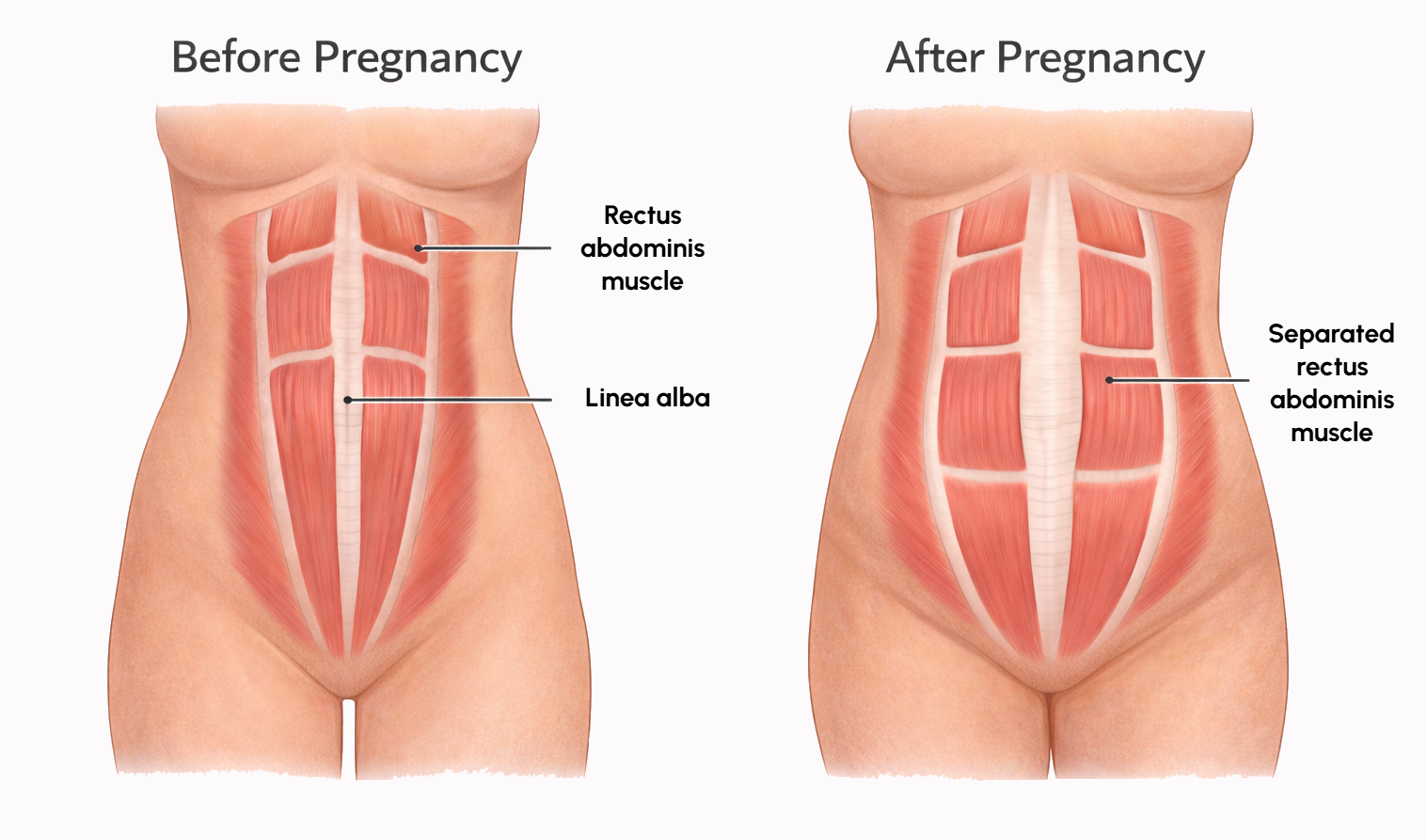
Abdominal Muscle Separation (Diastasis Recti / Rectus Diastasis)
Abdominal muscle separation (also known as ‘diastasis recti’ or ‘rectus diastasis’) refers to separation of the six-pack (rectus abdominis) muscles. During pregnancy, the growing uterus stretches the tissue (called the linea alba) between the six-pack muscles. In some women, this tissue does not fully recover, resulting in muscle separation. This causes the belly to protrude in the middle, especially when straining or sitting up. It can occur after C-section or vaginal delivery (often searched as diastasis recti after C-section). The bulge from diastasis recti is a generalised midline bulge rather than a localised shelf, and is sometimes described by patients as a “still-pregnant” or “rounded” abdomen.
In severe cases, women experience back pain or poor posture because the abdominal muscles aren’t providing the normal support. Physiotherapy can improve core function and sometimes reduce the separation, but significant diastasis often requires surgical repair for definitive correction.
Features suggestive of diastasis recti include:
- A generalised abdominal bulge, often more noticeable when sitting up or straining
- A feeling of reduced core strength
- A visible or palpable gap in the middle of the abdomen
- The bulge is not confined to the C-section scar area
Diastasis recti contributes to abdominal prominence but does not, on its own, cause a localised shelf at the scar. Many women with diastasis have no visible shelf, and many shelves occur without significant muscle separation.
To read more about abdominal muscle separation (diastasis recti) and how it is assessed in Sydney, see our Abdominoplasty (Tummy Tuck) page.
While muscle separation can contribute to abdominal prominence, it does not, on its own, explain a localised C-section shelf.
A C-Section Shelf Is Not Caused by Muscle Separation Alone
While diastasis recti can contribute to a generalised abdominal bulge, it does not typically produce a sharp, localised overhang directly above a C-section scar. Muscle separation affects the midline of the abdomen and becomes more apparent with straining or sitting up, whereas a shelf is defined by a fixed lower boundary at the scar itself.
Loose or Excess Skin After Pregnancy
Pregnancy can permanently stretch the abdominal skin, particularly in the lower abdomen. Once stretched beyond a certain point, skin does not reliably retract.
Common features include:
- Loose skin does not tighten with exercise
- Excess skin that folds over the C-section scar
- A soft bulge that persists despite weight normalisation
In addition, localized fat deposits may remain in the lower abdomen even in otherwise lean individuals. While fat contributes to abdominal fullness, fat alone is rarely the sole cause of a true C-section shelf.
In some patients, loose or hanging skin is not limited to a scar shelf but reflects more generalised excess skin after weight loss.
Clinical Assessment of Post-Pregnancy Abdominal Contour
During clinical assessment, surgeons typically evaluate:
- Scar quality and mobility
- Skin excess above and below the belly button
- The amount of fat and its distribution
- Presence and extent of abdominal muscle separation
How surgeons determine the cause of the bulge.
During assessment, three key questions are considered:
Is the prominence limited to the scar line or present across the entire abdomen?
Is the contour change caused by scar tethering, muscle separation, excess skin, or fat distribution?
Identifying the primary contributor helps determine whether scar revision, muscle repair, or abdominoplasty is the most appropriate treatment.
This distinction is important, because treatments target specific anatomical problems.
A C-Section Shelf Is Not a Hernia
A C-section shelf is not the same as a hernia. A hernia involves a weakening in the abdominal wall (fascia) that allows tissue to protrude through it. This usually produces a soft bulge that may vary with coughing or straining and can be associated with discomfort.
In contrast, a C-section shelf is most commonly related to scar tethering, skin excess, or soft-tissue redistribution, with the abdominal wall remaining intact. While hernias can occasionally coexist with post-pregnancy abdominal changes, they are not the typical cause of a shelf-type deformity.
C-section shelf, C-section pouch, and “mum tum”— what’s the difference?
“C-section pouch” and “mum tum” are non-medical terms commonly used to describe persistent lower abdominal fullness or a lower abdominal fold after pregnancy. It can reflect loose skin, residual fat, abdominal muscle separation (diastasis recti), and sometimes a scar-defined overhang after a Caesarean section (a “C-section shelf”). Because the causes differ, the most effective treatment depends on whether the dominant issue is scar tethering, skin excess, muscle separation, or a combination.
How Bulges are Prioritised in Clinical Assessment
In clinical practice, post-pregnancy abdominal concerns are assessed by determining which anatomical layer is driving the visible deformity, rather than by focusing on the scar alone. Many patients presenting for assessment describe the appearance as a “C-section pouch”, even when the underlying cause is scar tethering, skin laxity, or abdominal muscle separation.
Scar mobility and skin behaviour are usually evaluated first, because a fixed scar with overlying mobile tissue frequently explains a localised shelf even in patients with good muscle tone. Muscle separation is then assessed to determine whether it contributes to global abdominal prominence or functional weakness. Fat distribution is considered last, as fat alone rarely explains a shelf-type deformity.
This layered assessment explains why two women with similar-appearing scars may require very different treatments, and why addressing only one anatomical factor often produces incomplete correction.
Why Imaging is Not Routinely Required
In most patients, a detailed physical examination is sufficient to identify scar tethering, skin laxity, and muscle separation. Imaging (such as ultrasound or CT scanning) may be considered selectively by surgeons where symptoms suggest an alternative diagnosis, such as a hernia, or where clinical findings are unclear.
Treatment Options and When They Are Used
The choice between different treatments such as scar revision, abdominoplasty (tummy tuck) and liposuction depends on which anatomical layers are contributing to the problem.
| Primary cause | Typical treatment |
|---|---|
| Scar tethering alone | Scar revision |
| Muscle separation (diastasis recti) | Muscle repair during abdominoplasty |
| Excess skin | Abdominoplasty |
| Combination of factors | Full abdominoplasty |
Considering treatment for a persistent abdominal bulge after pregnancy?
In some cases, a visible C-section shelf or pouch may result from a combination of scar tethering, muscle separation, and excess skin.
When these factors occur together, procedures such as abdominoplasty (tummy tuck) may be considered to address the underlying anatomical changes.
For patients in Sydney, assessment focuses on identifying the dominant anatomical cause and determining which treatment approach is appropriate.
In some cases, Medicare rebates may apply when strict criteria are met.
Learn more about tummy tuck surgery and how it may address post-pregnancy abdominal contour changes.

Surgery is generally considered once postpartum healing has progressed and weight is relatively stable, because abdominal contour can continue to change as tissues settle. Abdominoplasty is usually not performed at the time of Caesarean delivery due to different operative priorities and recovery demands.
A tummy tuck (abdominoplasty) often becomes the most effective option after a C-section when excess skin or bulging extends beyond the scar itself, abdominal muscle separation contributes to persistent prominence, and the scar acts as a fixed point defining a visible shelf — because no more limited procedure can correct all of these factors together.
Scar Revision Surgery
Scar revision focuses on the scar itself. The old C-section scar is removed and re-closed, releasing tethered or stuck tissue and improving scar appearance.
Scar revision may be appropriate when:
- The shelf is mild
- Skin quality is otherwise good
- There is minimal excess fat
- There is no significant diastasis recti
Scar revision can improve scar appearance and release tethered tissue. However, it does not remove excess skin, tighten the abdominal wall, or correct diastasis recti. For this reason, it is suitable only for a limited group of patients.
Mini Abdominoplasty (Mini Tummy Tuck After C-Section)
A mini abdominoplasty addresses the lower abdomen only, below the belly button.
It may be considered when:
- Excess skin and fullness are confined to the lower abdomen
- The C-section scar contributes to contour irregularity
- The upper abdomen remains relatively firm
- There is little or no muscle separation
What it does:
- Removes lower abdominal skin and fat
- Often removes the C-section scar as part of the excision
What it does not do:
- Tighten separated abdominal muscles
- Address excess skin above the belly button
If laxity extends above the belly button, a mini abdominoplasty will not address it. For this reason, mini abdominoplasty is appropriate only in carefully selected patients, and does not address the majority of post-C-section abdominal contour concerns seen in clinical practice.
Full Abdominoplasty (Tummy Tuck) with muscle repair
A full abdominoplasty treats the entire abdomen.
It may be appropriate when:
- Loose skin extends above the belly button
- Diastasis recti is present
- There is a combination of scar tethering, skin laxity, and muscle separation
During a full tummy tuck:
- Excess skin and fat are removed
- The abdominal muscles are repaired if separated
- The C-section scar is usually removed and replaced with a new, lower scar
A full abdominoplasty is the most comprehensive and most commonly required procedure for women with persistent abdominal contour changes after C-section. To read more about abdominoplasty surgery in Sydney, see our Abdominoplasty (Tummy Tuck) page.
In patients with more extensive skin laxity extending beyond the abdomen, a body lift procedure may be considered.
Liposuction
Liposuction removes fat but does not address scar tethering, loose skin, or muscle separation.
It may be appropriate when:
- Skin quality is good
- There is no scar-related indentation
- Muscle separation is minimal or absent
In patients with a C-section shelf, liposuction alone often fails to correct the contour abnormality and may worsen the appearance if excess skin remains. For this reason, liposuction alone is rarely sufficient for a true C-section shelf.
Why One Treatment Alone May Not Fix The Problem
Post-pregnancy abdominal contour changes often involve more than one anatomical layer. For example, releasing a tethered scar may improve indentation but not address excess skin, while repairing muscle separation may improve abdominal support but leave a visible lower fold if skin laxity is present. This is why treatment planning considers scar behaviour, skin excess, fat distribution, and muscle separation together, rather than in isolation. Conservative measures can still improve comfort and core control, even if they don’t correct a C-section shelf.
Post-pregnancy abdominal contour changes often involve several anatomical layers at the same time:
| Layer involved | What happens |
|---|---|
| Skin | Stretched skin may fold above the scar |
| Muscle | Diastasis recti allows the abdomen to protrude |
| Fat | Fat adds volume but rarely explains the shelf alone |
Because these layers interact, correcting only one component may leave a visible contour change.
Exercise and Weight Loss Cannot Release a Tethered Scar
Exercise and weight loss cannot release a tethered C-section scar. A tethered or stuck C-section scar acts as a fixed point within the lower abdomen. While exercise can improve muscle tone and weight loss can reduce overall fat volume, neither can change the way scar tissue adheres to deeper layers. As a result, the overlying skin and soft tissue may continue to fold or overhang at the scar line despite significant fitness or weight changes.
What exercise can and cannot change
| Exercise can improve: | Exercise cannot: |
|---|---|
| Abdominal muscle strength | Release a tethered scar |
| Core stability | Remove excess abdominal skin |
| Posture | Reposition the C-section scar |
This is why a persistent shelf may remain even in very fit patients.
In some cases, weight loss can make a shelf more noticeable if skin laxity remains and the scar continues to anchor the lower abdominal contour.
Why Different Women Need Different Treatments for the Same “Shelf” Appearance
Women with a similar-appearing lower abdominal bulge may require different treatments because the underlying anatomy is not the same. In some patients, the primary issue is a fixed or indented scar with otherwise good skin quality and muscle tone. In others, the shelf reflects excess lower abdominal skin, muscle separation, or a combination of these factors. Treating only one layer without addressing the others often produces incomplete correction.
For this reason, treatment selection is based on identifying which anatomical layers are contributing most to the contour abnormality, rather than on the appearance of the scar alone.
This is why, in many post-C-section patients, a full abdominoplasty becomes the only procedure capable of addressing all contributing layers simultaneously.
Why a Tummy Tuck Is Often the Definitive Solution After a C-Section
When a post-pregnancy abdominal shelf or bulge is caused by more than one anatomical factor — such as a tethered C-section scar combined with excess skin and abdominal muscle separation — a limited procedure such as scar revision cannot correct all components.
A full abdominoplasty (tummy tuck) is specifically designed to address these problems together, by releasing scar tethering, removing excess skin, and repairing separated abdominal muscles in a single operation.
This is why, in many women after C-section, a tummy tuck is not simply one option among many, but the more definitive procedure capable of providing a complete and durable correction when multiple layers of the abdominal wall are involved.
Common Misconceptions about the C-section Shelf
Myth: Liposuction alone can fix a C-section shelf
Liposuction removes fat but does not release a tethered scar or tighten excess skin. In patients with a true shelf, liposuction alone often fails to correct the contour and may make the shelf more noticeable.
Myth: Rectus diastasis repair fixes a C-section shelf
Repairing abdominal muscle separation improves abdominal support but does not correct a scar-defined overhang. A shelf can persist even after successful muscle repair if skin laxity or scar tethering remains.
Myth: Fat freezing or non-surgical fat treatments can correct a shelf
Non-surgical fat treatments do not address scar behaviour or skin excess. Reducing fat volume without addressing tethering may worsen contour irregularity.
Myth: It will always go away with time
Early swelling can settle over months, but persistent shelves driven by scar tethering or skin excess may remain long-term.
Frequently Asked Questions
Understanding the C-section shelf
Is a C-section shelf fat or muscle?
A C-section shelf is neither purely fat nor purely muscle. In most cases, it is driven by scarring combined with excess skin, sometimes with a small contribution from underlying fat. Abdominal muscle separation (diastasis recti) may coexist, but muscle separation alone does not create a localized shelf at the scar. This is why weight loss or core exercises often have little effect on the shelf itself, even when overall abdominal tone improves.
Is a C-section pouch the same as a C-section shelf?
Yes. “C-section pouch” is a common patient term used to describe the same lower abdominal overhang that surgeons often refer to as a C-section shelf.
Is a C-section shelf a hernia?
No. A true C-section shelf is not a hernia. A hernia involves a weakness in the abdominal wall that allows tissue to protrude through it, often producing a soft bulge that may change with coughing or straining and may be associated with discomfort. A C-section shelf, by contrast, is most commonly caused by scar tethering, or excess skin above the C-section scar. The abdominal wall itself is usually intact.
In some women, an incisional or umbilical hernia can coexist with post-pregnancy abdominal changes, but this is not the typical cause of a shelf. Clinical examination — and occasionally scans — distinguishes between these conditions.
Understanding the cause
How can I tell which factor is dominant in my case?
The dominant factor is identified by where the bulge appears and how it behaves:
- Sharp ledge fixed at the C-section scar → scar tethering is dominant
- Broad midline bulge that worsens with straining or sit-ups → muscle separation is contributing
- Loose fold that collapses when bending forward → skin laxity is dominant
- Soft fullness without a defined step → fat contribution may be present
If a bulge changes markedly with coughing or straining, assessment is needed to exclude a hernia.
Why does my C-section shelf look worse when sitting?
A C-section shelf often appears more prominent when sitting because the scar remains fixed while the surrounding skin and soft tissue move. When the torso flexes (bends forward) during sitting, tissue above the scar falls forward, while a tethered or stuck C-section scar acts as a fixed point. This creates a visible step or overhang that is less apparent when standing upright.
How can I tell if it’s muscle separation or scar tethering?
Location is key. Muscle separation or rectus diastasis causes midline or generalised bulging; scar tethering causes a limited overhang directly above the scar.
Why doesn’t exercise fix this?
Exercise can improve muscle tone and function but cannot remove excess skin, release scar tethering, or close significant muscle separation.
Why does my tummy still look pregnant months or years after having a baby?
This can occur for different reasons. Some women have persistent skin laxity and a lower abdominal skin fold. Others have a degree of diastasis recti, which can cause central abdominal prominence, particularly with straining. A tethered C-section scar can also create a visible step or “ledge” at the lower abdomen. Identifying whether the issue is mainly scar-related, skin-related, muscle-related, or a combination helps determine what treatments are most appropriate.
Can a C-section shelf get worse over time?
It can become more noticeable with changes in weight, skin elasticity, or if scar tethering becomes more apparent as the scar matures. Many scars soften over time; however, the shelf appearance can persist if there is ongoing skin redundancy or a fixed scar line. This is one reason the assessment considers scar mobility, skin laxity, fat distribution, and any muscle separation together.
Treatment questions
Can scar revision alone fix a C-section shelf?
It can help when the shelf is caused mainly by scar tethering and surrounding tissues are otherwise firm. If excess skin or fat is present, scar revision alone is usually insufficient.
Is a tummy tuck the only real solution for a C-section shelf?
A tummy tuck is not always required, but it becomes the most effective solution when a C-section shelf is caused by a combination of scar tethering, excess skin, and abdominal muscle separation.
In these situations, limited procedures such as scar revision or liposuction address only part of the problem. A full abdominoplasty can correct all contributing layers at once.
Mini tummy tuck vs full tummy tuck after C-section — how is this decided?
The decision between a mini and full tummy tuck is based on how far the anatomical changes extend. If excess skin and contour irregularity are confined strictly to the area below the belly button, with no meaningful abdominal muscle separation, a mini abdominoplasty may be sufficient. If skin excess or bulging, and/or muscle separation extend above the belly button, a full abdominoplasty is usually required to achieve complete correction.
Will a tummy tuck remove my C-section scar?
In most cases, yes. The old scar is usually removed with the excess lower abdominal skin, and a new scar is created in a lower, more concealed position.
Do I need muscle repair if I have a bulge?
Muscle repair is usually required when diastasis recti is present and contributing to abdominal protrusion. It is performed as part of a full abdominoplasty, not often as a standalone procedure.
Can a C-section shelf be fixed without surgery?
Non-surgical treatments cannot reliably correct a true C-section shelf.
Exercise can improve core strength but cannot release a tethered scar or remove excess skin. Weight loss may reduce overall abdominal volume but often makes the shelf more visible if skin excess remains. Non-surgical fat treatments do not address scar fixation and may worsen contour irregularity.
Can diastasis recti be repaired without a tummy tuck?
In most cases, muscle repair is performed as part of an abdominoplasty because the overlying skin and contour also need to be addressed.
What is the difference between a C-section shelf and a “mum tum”?
A C-section shelf is typically localised and scar-related. A “mum tum” is a broader term that may include muscle separation, loose skin, or fat.
Can a C-section pouch go away without surgery?
In some cases, mild changes may improve over time, particularly early after pregnancy. However, when a C-section shelf is caused by scar tethering, excess skin, or significant muscle separation, it typically does not fully resolve with exercise or weight loss alone. Treatment depends on the underlying cause and may involve surgical options.
Putting It All Together
Post-pregnancy abdominal contour changes, including the C-section shelf, result from different anatomical causes. Scar behaviour, muscle separation, skin laxity, and fat distribution each require different treatments.
| Main issue | Typical treatment |
|---|---|
| Scar tethering only | Scar revision |
| Lower abdominal skin excess | Mini tummy tuck |
| Skin + muscle separation | Full tummy tuck |
If you are exploring surgery, understanding when Medicare may apply can help guide decision-making.
Effective treatment depends on accurately identifying which structures are involved.
Understanding these distinctions allows patients to make informed decisions and sets realistic expectations. Because different anatomical factors can produce a similar appearance, effective management depends on identifying the dominant underlying cause.
For patients in Sydney and the North Shore, this assessment process is an important part of planning any post-pregnancy abdominal surgery.
This information is general in nature and does not replace medical advice. A clinical assessment is required to determine which options, if any, may be appropriate.
About the Author
Dr Varun Harish is a Specialist Plastic, Reconstructive and Burns Surgeon in Sydney and a Fellow of the Royal Australasian College of Surgeons (FRACS) whose clinical practice includes abdominal wall surgery and post-pregnancy body contour surgery.
Dr Harish assesses patients with abdominal contour changes after pregnancy, including problems that can develop after Caesarean section such as C-section scar tethering, lower abdominal bulging, rectus diastasis (abdominal muscle separation), and excess skin or fat in the lower abdomen.
Patients often seek assessment for what is commonly described as a “C-section shelf” or “C-section pouch”, where the Caesarean scar creates a visible step or overhang in the lower abdomen. Treatment depends on the underlying cause and may include C-section scar revision, liposuction, rectus diastasis repair, or tummy tuck (abdominoplasty) surgery.
This article reflects Dr Harish’s clinical experience evaluating abdominal contour concerns after pregnancy and explaining the appropriate surgical and non-surgical treatment options.
Dr Varun Harish is the 2026 recipient of the Dr Ray Hollings Surgical Excellence Award, presented by Northern Sydney Local Health District.
You can learn more about Dr Varun Harish here.
Medical information in this article was prepared by Dr Varun Harish FRACS
Specialist Plastic, Reconstructive & Burns Surgeon – Sydney
Serving patients across the North Shore, Northern Beaches, Inner West and Central Coast.
Last reviewed: April 2026.
This article follows the clinical accuracy and editorial standards outlined in our Medical Content Standards policy.