Reconstruction After Skin Cancer Surgery: Who Repairs the Wound and How?
Dr Varun Harish, FRACS Plastic Surgeon
First published:
Hearing that you need skin cancer surgery can feel worrying, particularly when the cancer occurs on the face. Many patients are concerned not only about removing the cancer itself, but also about what happens afterwards. After a skin cancer has been removed, the remaining wound is repaired using stitches, a skin graft, or a local flap depending on its size and location.
Common questions include:
- Will there be a hole left after skin cancer removal?
- How will the wound be repaired?
- Who performs the reconstruction?
What Is Skin Cancer Reconstruction?
Skin cancer reconstruction refers to the surgical repair of the wound (defect) left after a skin cancer has been removed. The goal is to restore skin coverage while preserving function and achieving the best possible cosmetic outcome.
This process may also be described as repair of the surgical defect after skin cancer excision.
What Determines How a Skin Cancer Wound Is Repaired?
Once a skin cancer has been removed, the surgeon assesses the area (wound) that remains and determines how the wound should be repaired. Patients often describe this as a hole after skin cancer removal, although surgeons usually refer to it as a wound or surgical defect.
Several factors influence this decision:
- the size of the defect
- the location on the body or face
- the amount of nearby skin available
- whether surrounding structures need protection
- confirmation under the microscope that the cancer has been completely removed
Small wounds may be stitched together. Larger or more complex wounds may require reconstruction using a skin graft or a local skin flap. In many cases the same doctor removes the cancer and repairs the wound, although complex cases may be reconstructed by a plastic surgeon.
The best repair is the one that removes the cancer safely first, then closes the wound in a way that protects nearby structures and gives the most appropriate functional and cosmetic result for that body site.
In most cases the repair can be performed immediately. In other situations reconstruction may be delayed until laboratory testing of the removed tissue confirms the cancer margins are clear. If you would like to understand skin cancer margins and the pathology report see our article here.
Who Repairs the Wound After Skin Cancer Removal or Mohs Surgery?
In many cases, the doctor who removes the skin cancer also repairs the wound immediately after the cancer has been removed. This is common for smaller or straightforward lesions where the wound can be closed with stitches.
In other situations—particularly when the wound is larger, involves delicate facial structures, or requires more advanced reconstruction—a plastic surgeon may perform the repair. Plastic surgeons are trained to reconstruct skin defects while preserving both function and appearance. This situation commonly occurs after Mohs skin cancer surgery, where a Mohs surgeon removes the cancer layer-by-layer and a plastic surgeon may perform the reconstruction once clear margins have been confirmed. For this reason, some patients specifically search for a plastic surgeon after Mohs surgery when the wound is larger or in a delicate facial area.
Plastic surgeons are often involved when:
- the defect is large
- the cancer involves the face including the nose, eyelids, lips or ears
- the cancer involves the hands or legs
- stitching the skin back together (‘direct closure’) would distort nearby structures
- reconstruction requires skin grafts or local flaps
- both cosmetic and functional outcomes are important
Some suspicious lesions may initially be removed using minor skin surgery, while more complex cancers may require wider excision and reconstruction.
Considering reconstruction after skin cancer removal?
If you have been advised to undergo skin cancer removal and are unsure how the wound will be repaired, an assessment by a reconstructive surgeon can help clarify the most appropriate approach.
Dr Varun Harish is a specialist plastic and reconstructive surgeon in Sydney who performs skin cancer surgery and reconstruction of the face, nose, eyelids, ears, hands and lower limbs.

 At a glance: Reconstruction Options After Skin Cancer Removal
At a glance: Reconstruction Options After Skin Cancer Removal
 At a glance: Reconstruction Options After Skin Cancer Removal
At a glance: Reconstruction Options After Skin Cancer Removal| Technique | When Used |
|---|---|
| Direct closure | Small wounds with flexible skin |
| Skin graft | Larger shallow defects |
| Local flap | Complex or visible areas |
| Secondary intention | Selected wounds in certain locations |
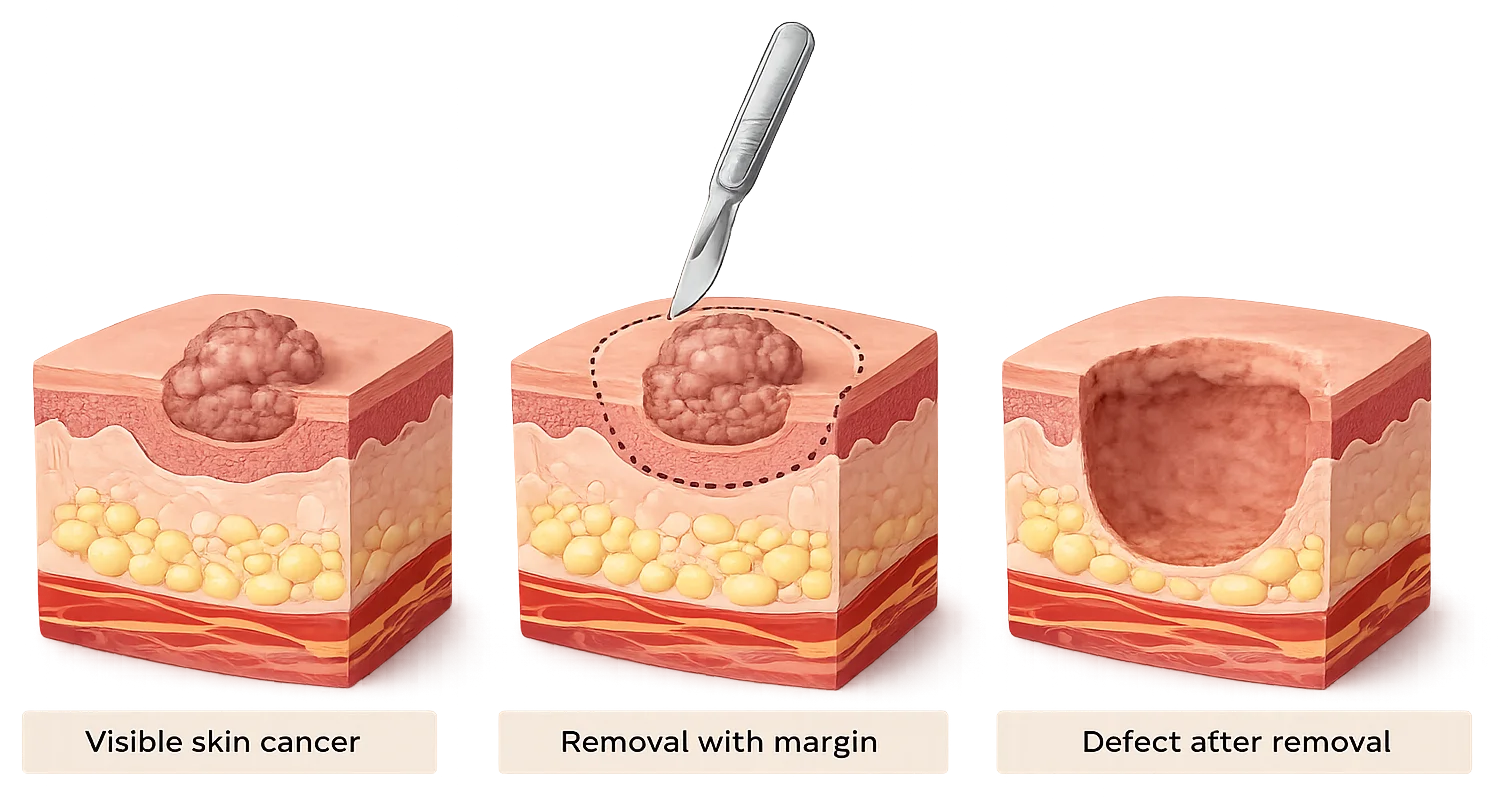
What Happens After Skin Cancer Is Removed?
The visible cancer and a surgical margin of surrounding skin are removed, which is why the wound is often larger than expected.
The surgeon assesses the size, depth, location, nearby skin movement, and whether important structures such as the eyelid, lip, nostril or ear could be distorted.
Depending on the site and defect, repair may involve direct closure, a skin graft, or a local flap depending on the size and location of the defect.
Repair is often performed immediately, but may be delayed until margins are confirmed after pathology or Mohs surgery.
Repair is often performed immediately, but may be delayed until margins are confirmed after pathology or Mohs surgery.
Why Is the Wound Sometimes Larger Than the Visible Skin Cancer?
Patients are sometimes surprised that the wound after skin cancer removal is larger than the visible lesion. This occurs because surgeons remove a margin of surrounding normal skin along with the cancer to reduce the risk of leaving microscopic cancer cells behind.
The margin size depends on:
- the type of skin cancer (see our skin cancer page for more information about types of skin cancer)
- tumour size
- tumour depth
- how aggressive the cancer appears
This is why a small skin cancer can sometimes leave a wound that looks unexpectedly large once the full treatment margin has been removed.
If you would like to understand this concept further, read our article explaining why margins matter in skin cancer surgery.
Is Reconstruction Done at the Same Time as Skin Cancer Removal?
In many cases reconstruction is performed immediately after the cancer is removed. In other situations it may be delayed until pathology or Mohs assessment confirms that the cancer has been completely removed.
Immediate reconstruction
In many cases reconstruction is performed during the same operation as the cancer removal.
This is common when:
- margins are predictable
- the defect is small or moderate
- the repair technique is relatively straightforward
Delayed reconstruction
In some situations reconstruction may be delayed.
This can occur when:
- the visible ends of the cancer are difficult to see on the surface
- Mohs skin cancer surgery is used
Delaying reconstruction ensures the cancer has been completely removed before undertaking more complex repair. This is most relevant when the edges of the cancer are difficult to define, when the wound is in a cosmetically or functionally sensitive area, or when a more complex repair would be unwise before margins are confirmed.
How a Wound Is Repaired After Skin Cancer Removal
Once the cancer has been removed, several reconstructive options may be used depending on the size and location of the defect. The aim is to restore skin while preserving function and achieving the best possible cosmetic outcome.
The main methods of repair after skin cancer excision are direct closure, skin grafting, local flap reconstruction, and in selected cases healing by secondary intention.
How Surgeons Decide Which Repair Is Best
| Situation | Typical Repair | Why |
|---|---|---|
| Small wound with loose surrounding skin | Direct closure with stitches | Simplest option when the edges can be brought together without distortion |
| Larger shallow wound with limited nearby skin | Skin graft | Covers larger areas when surrounding skin cannot be stretched |
| Wound in a visible or complex area | Local flap | Uses nearby matching skin and may better preserve contour and function |
| Selected wounds in certain locations | Healing by itself (secondary intention) | Some wounds heal well without stitches |
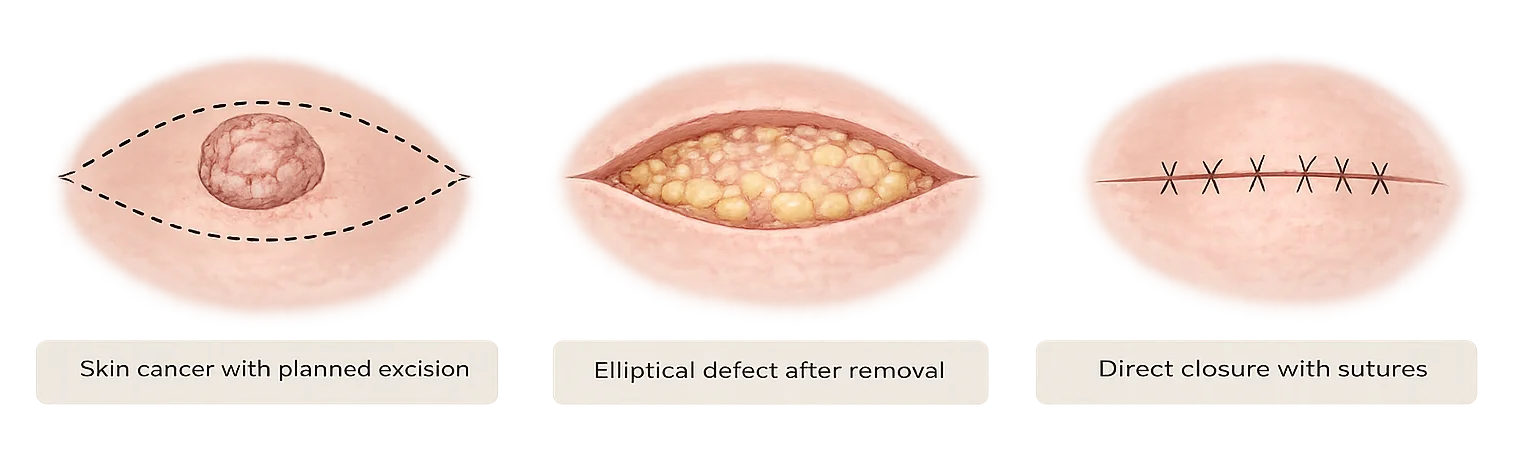
Direct Closure
Direct closure after skin cancer removal involves bringing the edges of the wound together with stitches.
This may be possible when:
- the defect is relatively small
- surrounding skin can be mobilised
- closure will not distort nearby structures
Areas such as the cheek often allow direct closure because the skin is more flexible.
Direct closure is usually the simplest repair when the wound edges can be brought together safely. However, direct closure is not always the best option. In some locations, closing the wound directly can place too much tension on the surrounding skin and distort nearby structures such as the eyelid, nostril, lip, or ear.
Skin Graft
A skin graft after skin cancer removal involves transferring a thin layer of skin from another part of the body to cover the wound.
Skin grafts may be used when:
- the wound cannot be closed directly
- surrounding skin is limited
- the defect is broad and shallow
They are commonly used on areas such as the nose, ear, or scalp.
Skin grafts may apply to reconstruction after BCC removal or reconstruction after SCC removal when the size and location of the wound make direct closure less suitable.

Grafts can be very useful when there is not enough nearby skin to close the wound directly. However, because the skin comes from a different site, a graft may not always match the surrounding colour, thickness, or contour as well as nearby skin moved with a flap.
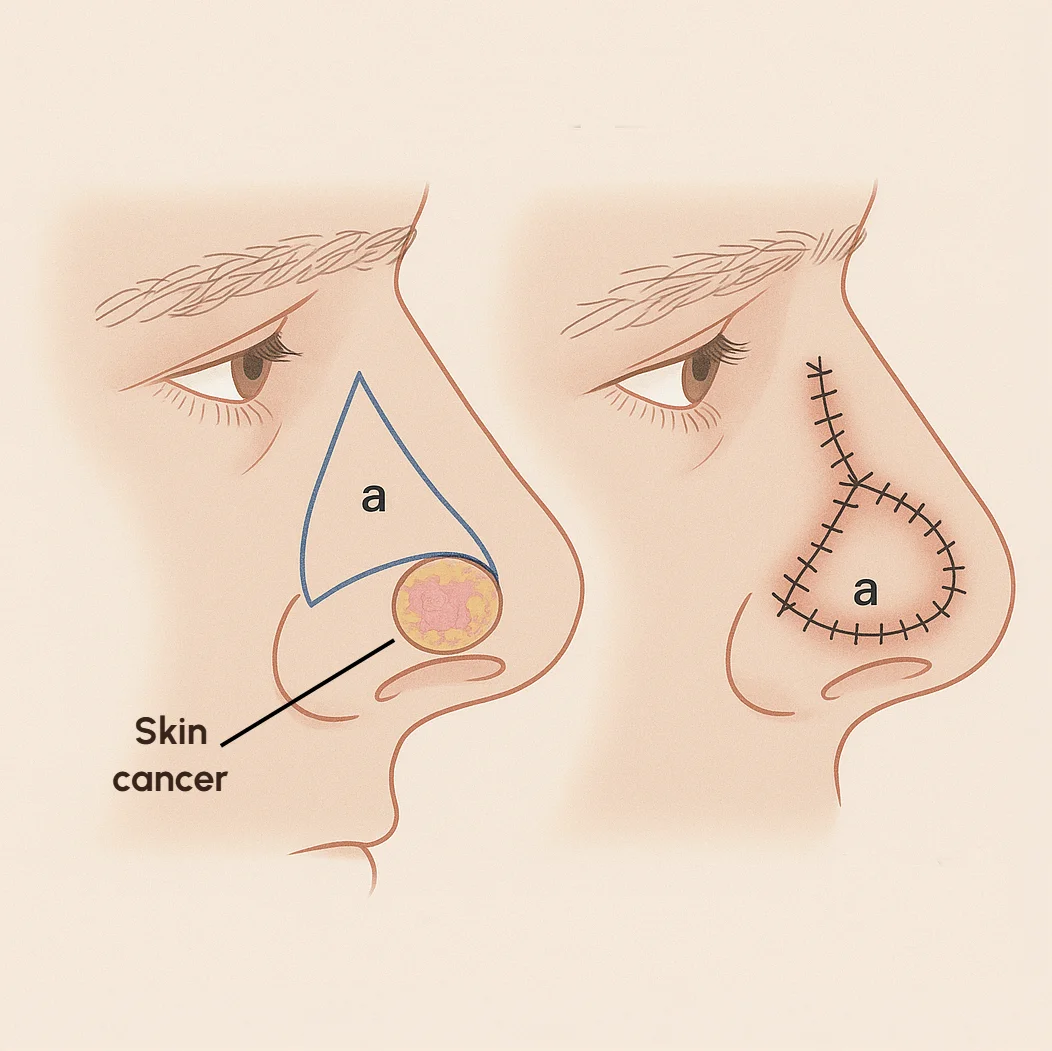
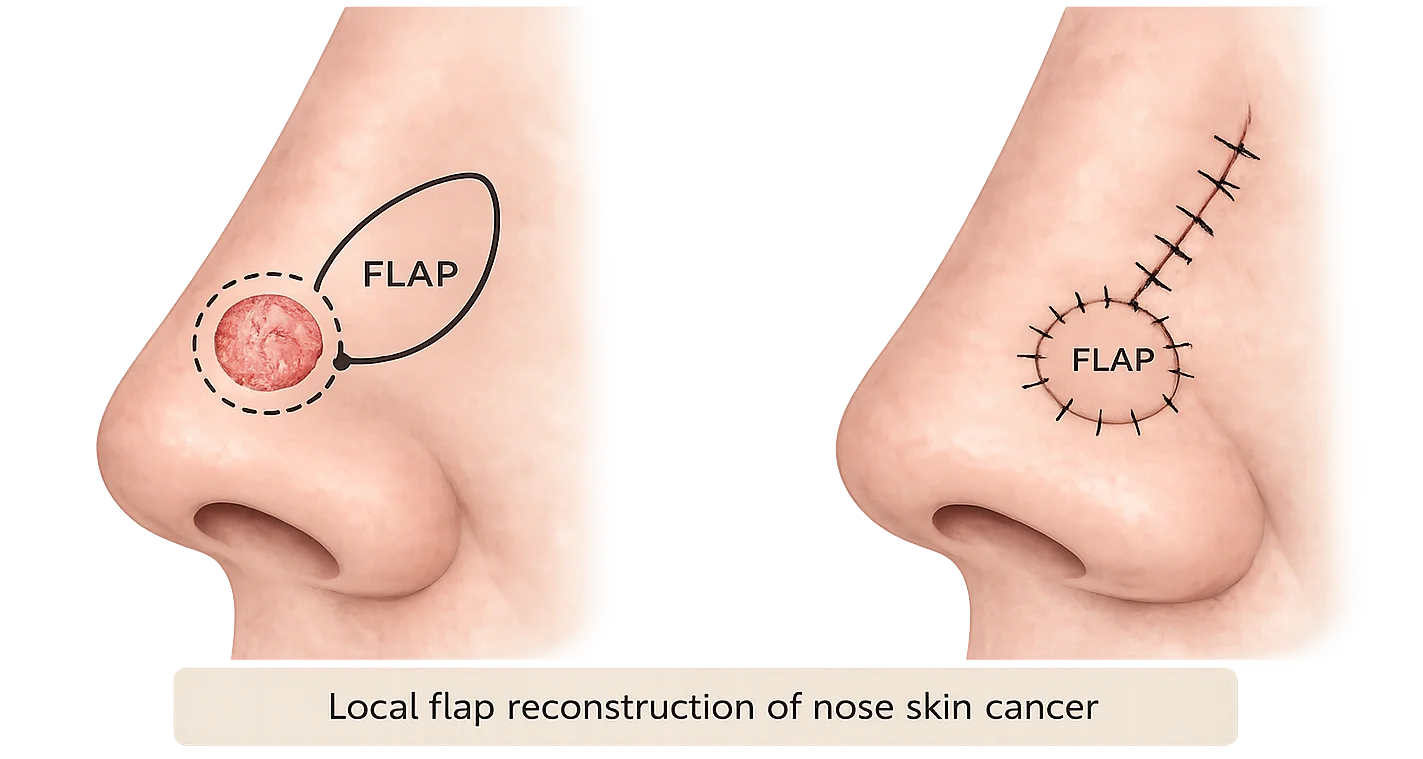
Local Flap
A local flap after skin cancer removal uses nearby skin that remains attached to its blood supply and is moved into the wound. Because this skin comes from next to the defect, it often provides a closer match in colour, thickness, and texture than a skin graft. This type of skin cancer flap surgery is often preferred in visible or functionally important areas because it may better match the surrounding colour, thickness, and contour.
Skin Graft vs Flap Reconstruction: What’s the Difference?
When a wound cannot be closed directly, surgeons may use either a skin graft or a local flap to repair the defect. The best option depends on the location of the wound, the amount of nearby skin available, and the functional and cosmetic needs of the area.
| Feature | Skin graft | Local flap |
|---|---|---|
| Tissue source | Skin taken from another area | Nearby skin repositioned |
| Blood supply | Relies on blood supply from wound bed | Maintains its own blood supply |
| Cosmetic match | May differ slightly | Often better match |
| Typical locations | Neck, ear | Face, nose, cheek, lip |
In general, grafts are useful for covering a wound when there is insufficient local skin, while flaps are often preferred in visible or functionally important areas because they may better preserve contour, movement, and skin match. For many facial skin cancers, local flap reconstruction may provide a more natural cosmetic outcome, although grafts remain an important option.
In reconstruction after skin cancer surgery, the best repair is not always the simplest-looking option on paper. A short straight-line closure may seem attractive, but if it places too much tension on the surrounding skin it can distort nearby structures or produce a poorer long-term result. In many cases, a graft or flap is chosen not because the wound is impossible to close, but because it offers a safer or more natural reconstruction for that particular site.
How Do I Know Which Reconstruction I Need?
- Small wound with loose skin → often direct closure
- Larger broad wound → may need graft
- Visible area needing skin match → may need local flap
- Complex facial site or uncertain margins → repair may be delayed until pathology or Mohs clearance
Reconstruction After Mohs Skin Cancer Surgery
Mohs surgery removes skin cancer in stages while examining each layer under a microscope.
Once the final stage confirms the cancer has been completely removed, reconstruction can be performed.
Repair may involve:
- direct closure
- skin grafts
- local flap reconstruction
This repair following Mohs surgery is sometimes referred to as Mohs reconstruction and is often performed by a plastic surgeon. This type of repair may also be referred to as Mohs defect reconstruction or Mohs wound repair.
Facial Reconstruction After Skin Cancer Surgery
Facial reconstruction after skin cancer is different from reconstruction elsewhere on the body because each part of the face has different cosmetic and functional demands. Reconstruction after facial skin cancer removal aims not only to close the wound, but also to preserve important functions such as breathing, blinking, speech, eating, and normal facial symmetry. In simple terms, facial reconstruction after skin cancer aims to remove the cancer safely while restoring normal appearance and function.
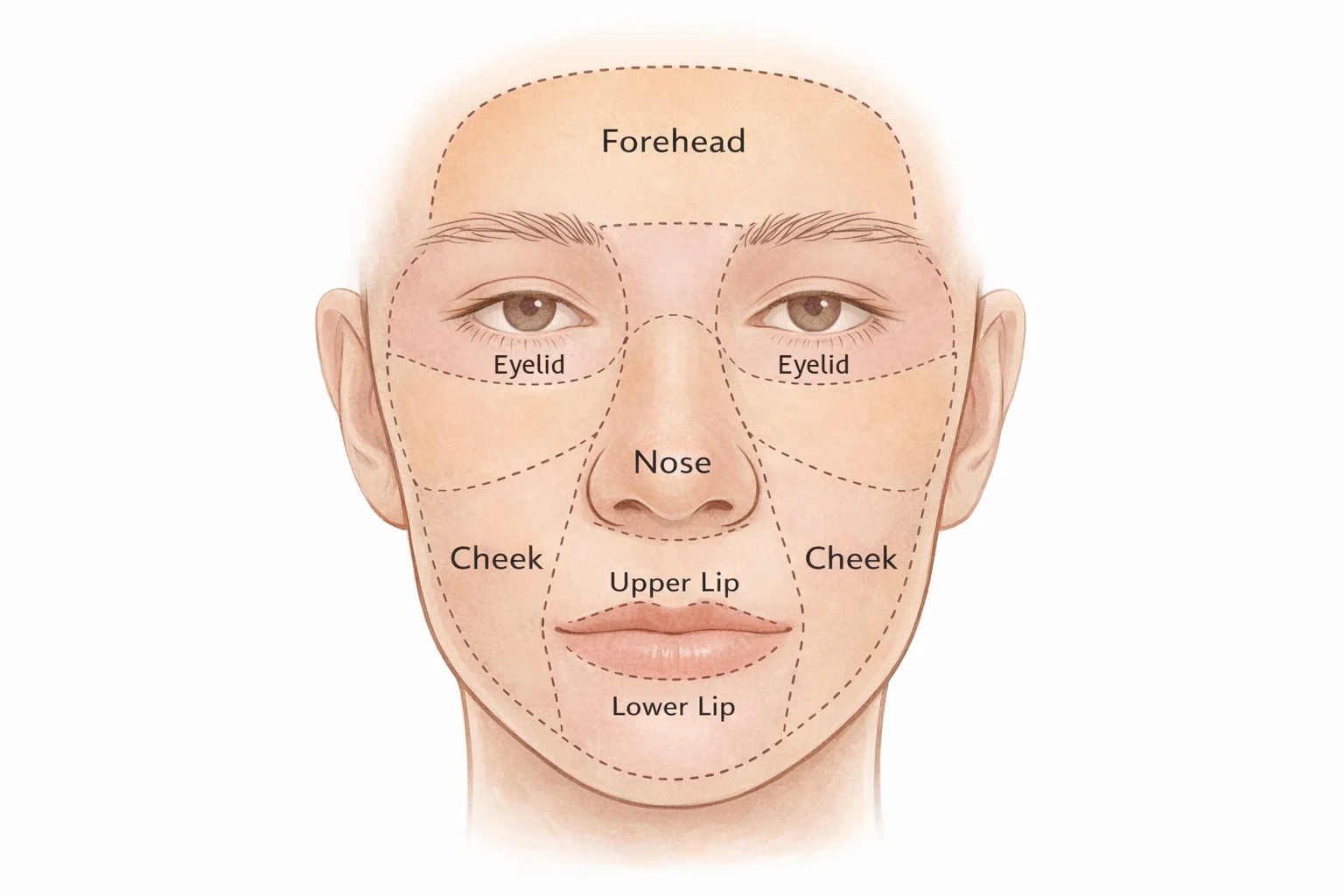
Surgeons often plan facial reconstruction after skin cancer surgery using the concept of facial aesthetic units—natural sub-regions of the face where scars and tissue movement can often be placed more discreetly. This helps surgeons place scars more discreetly, borrow skin from the most suitable nearby area, and avoid pulling on important facial structures.
The best reconstructive approach depends on the exact facial site, the size of the wound, the amount of nearby skin available, and the function that needs to be preserved. Depending on the size and location of the wound, reconstruction may involve direct closure, skin grafts, or local flap techniques that move nearby skin to repair the defect.
Where Is the Skin Cancer?
The best reconstruction depends heavily on where the skin cancer is located, because each part of the face and body has different functional and cosmetic priorities. Different parts of the face and body behave differently after reconstruction, which is why the same repair method may produce very different outcomes depending on the location. Reconstruction on the face often prioritises contour and function, while reconstruction on the body may prioritise durability and wound healing.
Select an area below to see how reconstruction differs.
Skin Cancer Removal on the Nose
Skin cancer on the nose is one of the most common reasons patients require facial skin cancer surgery and reconstruction. After skin cancer removal on the nose, reconstruction aims to restore the natural shape of the nose while preserving normal breathing and matching surrounding skin thickness and colour. This is why nose reconstruction after skin cancer, including reconstruction after BCC or SCC removal on the nose, often requires more planning than patients expect.
Because nasal skin is relatively tight and the nose has complex contours, larger defects often require local flap reconstruction rather than simple stitches. These flaps allow nearby skin with similar colour and thickness to be moved into the area, helping restore the natural shape during nose reconstruction after skin cancer.
On the nose, the skin has unique thickness, contour, and sebaceous quality. For this reason, simply patching the area with a graft may not always recreate the natural shape or skin match as well as a carefully planned local flap.
Skin Cancer Removal on the Eyelid
Skin cancer on the eyelid requires particularly careful reconstruction because the eyelids protect the eyeball, help maintain lubrication of the eye and allow normal blinking. Repair aims to maintain:
- the ability to close the eye fully
- normal blinking
- protection of the eye
Because the eyelid is such a delicate functional structure, even a relatively small defect can have a disproportionate effect on comfort, eye protection, and appearance. Eyelid reconstruction after skin cancer therefore focuses on restoring the edge of the eyelid and its normal shape, so that the eye continues to close comfortably and remain protected. Careful repair is important to avoid eyelid pulling downward (called ‘ectropion’) or insufficient closure.
For more information about eyelid skin cancer removal and reconstruction, see our skin cancer surgery procedure page.
Skin Cancer Removal on the Cheek
Cheek reconstruction after skin cancer often takes advantage of the flexibility of cheek skin. For this reason, skin cancer removal on the cheek may frequently be repaired with direct closure using stitches. Even so, scar direction and tension still matter, particularly near the lower eyelid, nose, or lip.
When the wound is larger, local flap techniques may be used to reposition nearby skin while keeping scars aligned with natural facial lines, helping them blend in more naturally.
Surgeons often use rhomboid and advancement flaps on the cheek because the surrounding skin allows tissue to be moved while maintaining a natural facial contour.
Skin Cancer Removal on the Lip
Reconstruction after skin cancer on the lip must preserve both appearance and function. The lips are essential for speech, eating, drinking, and facial expression.
Surgical repair aims to maintain:
- lip symmetry
- normal speech
- comfortable eating and drinking
The lip contains a circular muscle (‘orbicularis oris’) that controls lip movement. Lip reconstruction after skin cancer must preserve this muscle so that speech, eating, and lip closure remain normal. Additionally, lip reconstruction involves carefully aligning the border between the pink lip and the surrounding skin, so the lip looks natural and moves normally. Even small misalignment at the lip border can be noticeable.
Skin Cancer Removal on the Ear
The ear contains cartilage that provides its distinctive shape. Reconstruction after skin cancer on the ear must preserve this cartilage framework so the ear keeps its normal contour.
Skin cancers on the ear sometimes require removal of a small portion of cartilage. Because the ear has a complex three-dimensional shape, reconstruction often focuses on preserving the natural contour of the ear rim and surrounding cartilage. Ear reconstruction after skin cancer may involve skin grafts or local flap techniques to restore both skin coverage and shape.
Skin Cancer Removal on the Forehead
Skin cancer on the forehead is also common because this area receives significant sun exposure. The forehead skin is relatively mobile, which means skin cancer removal on the forehead can often be repaired with direct closure.
For larger defects, nearby skin may be repositioned using flap techniques so the scar follows the natural horizontal lines of the forehead and avoids distortion of the eyebrows or hairline. Forehead reconstruction after skin cancer often focuses on balancing a straightforward closure with careful scar placement in a highly visible part of the face.
For these reasons, reconstruction after facial skin cancer surgery is usually tailored to the exact facial location, the size of the wound, and the function that needs to be preserved. The key differences between facial sites are summarised below.
| Facial site | Key reconstructive considerations | Common reconstruction approach |
|---|---|---|
| Nose | Preserving nasal contour, breathing, and skin thickness match | Often local flap reconstruction rather than direct closure with stitches; occasionally a skin graft depending on defect size |
| Eyelid | Protecting the eye, maintaining normal blinking and preventing ectropion (eyelid distortion) | Eyelid reconstruction using local flap techniques wherever possible to restore eyelid support and prevent distortion |
| Cheek | Flexible skin allows tension to be redistributed | Direct closure with stitches or local flap depending on wound size |
| Lip | Maintaining lip symmetry, speech, and eating function | Reconstruction that restores muscle alignment and the natural lip border |
| Ear | Preserving cartilage shape and ear contour | Skin grafts or local flaps depending on defect size |
| Forehead | Visible scars and eyebrow position must be preserved | Direct closure with stitches or flap techniques aligned with forehead lines to prevent eyebrow or hairline distortion |
Skin Cancer Reconstruction on the Hands and Legs
Skin cancers can also occur on the hands and legs, and reconstruction in these areas presents different challenges compared with the face.
Reconstruction after skin cancer removal on the lower leg can be more challenging than on many other parts of the body because the skin is tight, the blood supply may be less forgiving, and swelling is common. For this reason, wounds on the shin or lower leg are often less suitable for simple direct closure than patients expect.
Depending on the wound, reconstruction after skin cancer removal on the hands or legs may involve:
- direct closure with stitches
- skin graft after skin cancer removal on the leg or hand
- local flap techniques using nearby skin
Skin on the lower leg is tighter and has a relatively reduced blood supply compared with the face, which means wounds in this area may sometimes require grafts or flap reconstruction to support reliable healing.
For skin cancer on the leg surgery, direct closure with stitches is sometimes possible if the wound is small and the surrounding skin can be mobilised. Skin grafts are commonly used on the lower leg when the wound is broad and there is not enough surrounding skin to close the area safely without excessive tension.
On the hand, reconstruction must protect movement, maintain durable skin cover, and avoid restricting nearby joints or tendons. Even when the wound is small, preserving function remains a key priority.
Because movement, swelling, and reduced skin laxity can affect healing in the limbs, the best reconstructive option is often the one that balances reliable wound healing with function and acceptable scarring, rather than simply the shortest operation.
What Affects the Final Scar After Skin Cancer Surgery?
For many patients, one of the main questions after reconstruction is what the scar will look like after skin cancer removal.
Several factors influence how the final scar appears after skin cancer surgery. These include:
- the size of the surgical defect
- the location on the face or body
- the amount of surrounding skin available
- the reconstruction technique used
- individual healing characteristics
In general, scars are easier to hide when they can be placed along relaxed skin lines or natural facial sub-units. Direct closure may produce a fine linear scar when tension is low, whereas grafts and flaps may be necessary when simple closure would distort nearby structures. Importantly, the best scar is not always the shortest scar. In many cases, a longer but carefully planned reconstruction produces a better functional and cosmetic result than a short closure performed under excessive tension.
Recovery after Skin Cancer Reconstruction
Most wounds heal soon after surgery. Scars often look firmer, redder, or more noticeable early on, then gradually soften and fade over several months.
Recovery may include:
- wound care
- scar massage
- sun protection
- follow-up monitoring
The exact recovery depends on the size and location of the wound, whether a graft or flap was used, and how well the area can be protected during healing. In some cases further procedures such as scar revision surgery may improve the final appearance.
Recovery after skin cancer reconstruction often differs depending on whether the wound is closed directly, covered with a skin graft, or repaired using a local flap. Direct closure, skin grafts and local flaps can all heal well, but dressings, swelling, scar maturation and follow-up needs may differ depending on the method used and the location of the wound.
| Repair type | Typical early healing | Dressings / wound care | Scar / contour considerations | Follow-up considerations |
|---|---|---|---|---|
| Direct closure (simple stitches) | Usually the simplest recovery if the wound edges can be brought together without too much tension. Mild swelling, bruising and tightness are common early. | Usually involves a straightforward dressing and routine wound care until stitches are removed or dissolve. | Leaves a linear (straight) scar. Final scar quality depends on wound tension, location, skin quality and individual healing. | Follow-up is often focused on wound care and scar maturation. |
| Skin graft (skin taken from another site) | Early healing depends on how well the graft “takes” to the wound bed. Colour and texture may look different from the surrounding skin at first. | Dressings are usually left in place for several days (often around 5–7 days) to protect the graft while it establishes its blood supply. Both the graft site and donor site may need care. | Grafts may have a different colour, thickness or contour from adjacent skin, particularly on the face or lower leg. | Follow-up often focuses on graft take, wound care, and how the donor site is healing. |
| Local flap (nearby skin repositioned) | Swelling and bruising may be more noticeable early because nearby tissue has been moved to repair the defect. | Dressings and wound care are typically similar to direct closure (simple dressing). | Local flaps often provide a better skin match and contour than a graft, but scars may be longer. | Follow-up often focuses on flap healing, scar placement, contour, swelling, and any staged adjustments if needed. |
Local flaps are often preferred on the face because they use nearby skin with similar colour and texture, which may help preserve natural contours. Skin grafts are often used when there is not enough nearby skin to close the wound directly.
The exact recovery pattern still depends on the size and location of the wound, whether the reconstruction is on the face or body, and individual factors such as skin quality, circulation, smoking status and scar tendency. In other words, two patients who both have a flap or a graft may still heal differently depending on the defect and the reconstructive goals.
Practical point
Direct closure often has the simplest wound care. Skin grafts usually require closer early dressing protection. Local flaps may involve more swelling early on, but may offer better colour and contour match in selected areas.
Frequently Asked Questions
Who repairs the wound after Mohs surgery?
The Mohs surgeon may repair the wound, particularly if the defect is small and straightforward. In more complex cases, reconstruction may be performed by a plastic surgeon once clear margins have been confirmed.
Will I have a hole after skin cancer removal?
Once the cancer has been removed, a wound or defect is left in the skin. This may be closed directly with stitches, repaired with a skin graft, or reconstructed with a local flap depending on the size, location, and complexity of the wound.
Can a plastic surgeon remove skin cancer?
Yes. Plastic surgeons are trained in both skin cancer removal and reconstruction, particularly when the cancer is in a cosmetically or functionally important area.
How big will the scar be after skin cancer removal?
The scar is often larger than the visible skin cancer because surgeons remove a margin of surrounding skin to ensure complete treatment. The final scar also depends on the body site, the amount of surrounding skin available, and the type of reconstruction used.
Is reconstruction done at the same time as cancer removal?
Often it is. In some situations reconstruction is delayed until pathology or Mohs assessment confirms that the cancer has been completely removed before a more complex repair is undertaken.
How long does reconstruction take to heal?
Initial wound healing usually occurs over several weeks, but scars continue to mature over several months. Recovery varies depending on the size and location of the wound and whether the reconstruction involved direct closure, a graft, or a flap.
Will I need a skin graft after skin cancer removal?
Not always. Many skin cancers can be removed and closed directly with stitches. Skin grafts are usually considered when the wound is larger or when there is not enough surrounding skin to close the area safely without excessive tension.
What will the scar look like after skin cancer removal?
The final scar after skin cancer removal depends on several factors including the size of the cancer, the surgical margin required for safe removal, the location on the body, and the type of reconstruction performed. In many cases the scar is larger than the visible cancer because surgeons remove a margin of surrounding skin to ensure the cancer has been completely treated. Surgeons aim to place scars along natural skin lines or facial sub-units where possible to make them less noticeable. Scars typically continue to soften and fade over several months as healing progresses.
Key Takeaway
After skin cancer removal, the wound may be repaired in several ways depending on its size and location. Small wounds may be closed directly, while larger defects may require grafts or local flaps. Reconstruction aims to restore both function and appearance while ensuring the cancer has been completely treated.
Questions about reconstruction after skin cancer surgery?
Every skin cancer and every wound is different.
Reconstruction may involve direct closure, a skin graft, or a local flap depending on the location and size of the defect.
If you would like personalised advice about reconstruction options after skin cancer removal, a consultation can help clarify the safest and most appropriate approach.
About the Author
Dr Varun Harish is a Specialist Plastic, Reconstructive and Burns Surgeon in Sydney and a Fellow of the Royal Australasian College of Surgeons (FRACS).
Dr Harish has a particular interest in skin cancer surgery and reconstruction including Mohs surgery reconstruction. His research in skin cancer surgery has been published in peer-reviewed journals, and work from this research has been cited in international clinical skin cancer guidelines. He is involved in the management of skin cancer patients through multidisciplinary cancer teams at major cancer hospitals in Sydney, working with radiation oncologists, medical oncologists, dermatologists, and other specialists to plan optimal treatment.
This article reflects Dr Harish’s clinical experience performing skin cancer reconstruction after both standard excision and Mohs surgery, including complex reconstruction of the face, eyelids, nose, lips, ears, hands and lower limbs.
Dr Varun Harish is the 2026 recipient of the Dr Ray Hollings Surgical Excellence Award, presented by Northern Sydney Local Health District.
You can learn more about Dr Varun Harish here.
Medical information in this article was prepared by Dr Varun Harish FRACS
Specialist Plastic, Reconstructive & Burns Surgeon – Sydney
Serving patients across the North Shore, Northern Beaches, Inner West and Central Coast.
Last reviewed: April 2026.
This article follows the clinical accuracy and editorial standards outlined in our Medical Content Standards policy.